
Dose-Response Relationship between Endurance Training Prescription Variables and Increases in Aerobic Performance of Healthy and Unhealthy Middle and Very Old Individuals Aged 70 Years and Older: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search Strategy
2.2. Risk of Bias Assessment
2.3. Inclusion and Exclusion Criteria
- Population: studies involving healthy and unhealthy (i.e., patients with heart failure and preserved ejection fraction, individuals with ischemic heart disease, hypertension, musculoskeletal problem, respiratory disease, diabetes, overweight or obese) middle and very old adults (aged 70 years and older).
- Intervention or exposure:
- Studies investigating the effects of ET on VO2peak in older adults;
- Comparator: Studies comparing an experimental group with a control group;
- Outcome(s):
- VO2peak (L/min or mL/kg/min);
- Training prescription variables: type of training, training frequency (sessions/week), and training duration (weeks);
- Study design: RCTs studies;
- Studies were excluded if:
- (i)
- Reviews, opinion papers and commentaries, interviews, editorials, posters, conference papers, letters to the editor, book chapters, and books.
- (ii)
- Articles with insufficient data.
2.4. Coding of Studies
2.5. Data Extraction
2.6. Statistical Analyses
3. Results
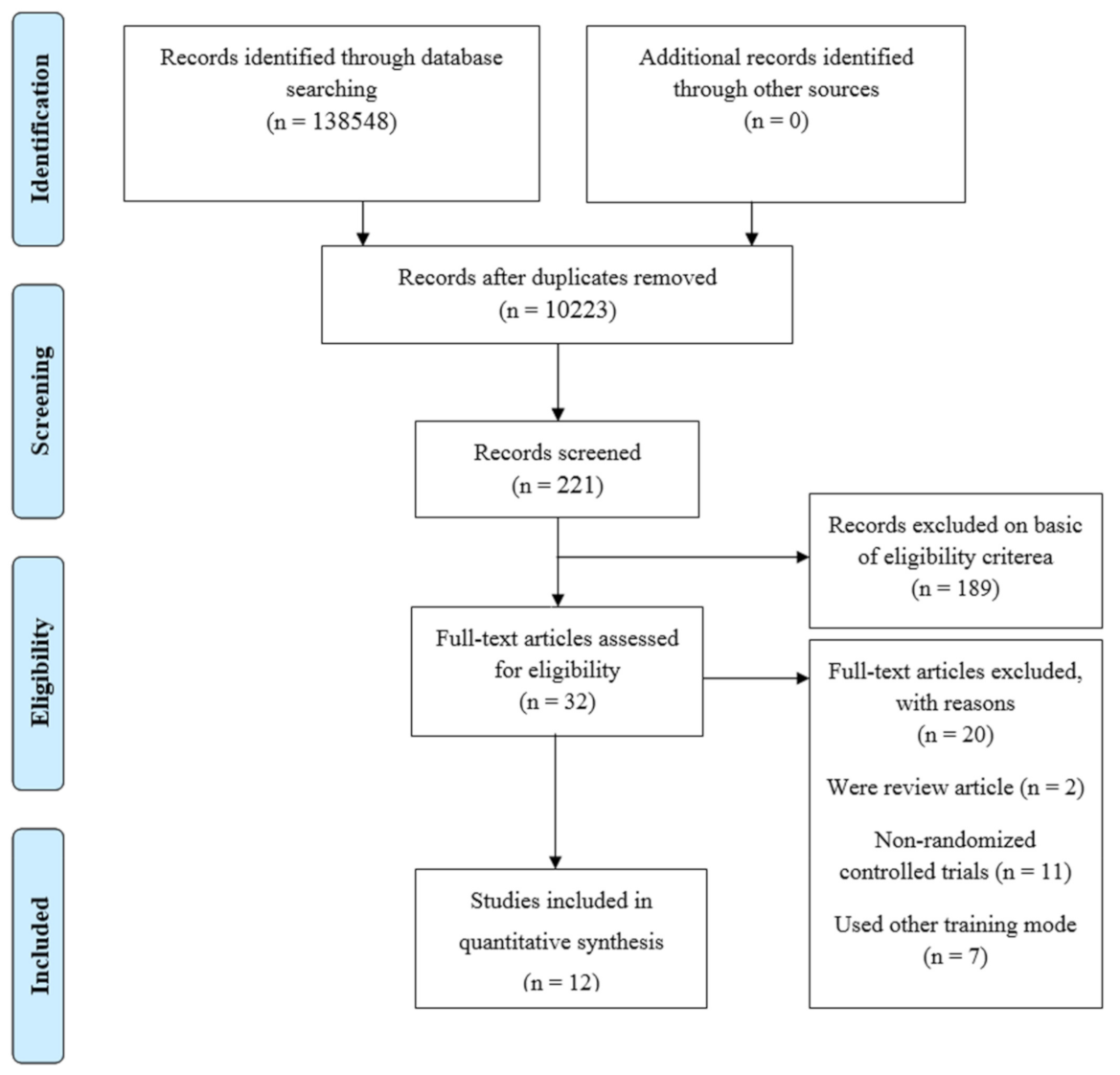
3.1. Literature Search Results
3.2. Overall Effects of Endurance Training on Measures of VO2peak
3.3. Influence of Different Moderating Variables on Endurance Training Related Effects
3.3.1. Health Status
3.3.2. Gender
3.4. Dose–Response Relationships of Endurance Training on VO2peak
3.4.1. Findings from the Meta-Regression
3.4.2. Findings from the Univariate Analysis
Training and Session Duration and Training Frequency
3.5. Evaluation of Publication Bias
4. Discussion
4.1. General Effectiveness of Endurance Training on VO2peak
4.2. Participants Characteristics
4.3. Dose–response Relationships of Endurance Training on VO2peak
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Watad, A.; Bragazzi, N.L.; Adawi, M.; Amital, H.; Toubi, E.; Porat, B.-S.; Shoenfeld, Y. Autoimmunity in the elderly: Insights from basic science and clinics—A mini-review. Gerontology 2017, 63, 515–523. [Google Scholar] [CrossRef] [Green Version]
- Knudson, R.J. How aging affects the normal lung. J. Respir. Dis. 1981, 2, 74–84. [Google Scholar]
- Steenman, M.; Lande, G. Cardiac aging and heart disease in humans. Biophys. Rev. 2017, 9, 131–137. [Google Scholar] [CrossRef]
- Mialet-Perez, J.; Douin-Echinard, V.; Cussac, D.; Bril, A.; Parini, A. Ageing: A matter of heart? Med. Sci. (Paris) 2015, 31, 1006–1013. [Google Scholar] [CrossRef] [Green Version]
- Seals, D.R.; Monahan, K.D.; Bell, C.; Tanaka, H.; Jones, P.P. The aging cardiovascular system: Changes in autonomic function at rest and in response to exercise. Int. J. Sport Nutr. Exerc. Metab. 2001, 11, S189–S195. [Google Scholar] [CrossRef]
- Miljkovic, N.; Lim, J.-Y.; Miljkovic, I.; Frontera, W.R. Aging of skeletal muscle fibers. Ann. Rehabil. Med. 2015, 39, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Hollmann, W.; Strüder, H.K.; Tagarakis, C.V.; King, G. Physical activity and the elderly. Eur. J. Cardiovasc. Prev. Rehabil. 2007, 14, 730–739. [Google Scholar] [CrossRef] [PubMed]
- Siparsky, P.N.; Kirkendall, D.T.; Garrett, W.E., Jr. Muscle changes in aging: Understanding sarcopenia. Sports Health 2014, 6, 36–40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, W.K.; Williams, J.; Atherton, P.; Larvin, M.; Lund, J.N.; Narici, M.V. Sarcopenia, Dynapenia, and the impact of advancing age on human skeletal muscle size and strength: A quantitative review. Front. Physiol. 2012, 3, 260. [Google Scholar] [CrossRef] [Green Version]
- Pereira, A.F.; Silva, A.J.; Costa, A.M.; Monteiro, A.M.; Bastos, E.; Marques, M.C. Muscle tissue changes with aging. Acta Med. Port. 2013, 26, 51–55. [Google Scholar]
- Clennin, M.N.; Payne, J.P.; Rienzi, E.G.; Lavie, C.J.; Blair, S.N.; Pate, R.R.; Sui, X. Association between cardiorespiratory fitness and health-related quality of life among patients at risk for cardiovascular disease in uruguay. PLoS ONE 2015, 10, e0123989. [Google Scholar] [CrossRef]
- Bouaziz, W.; Kanagaratnam, L.; Vogel, T.; Schmitt, E.; Dramé, M.; Kaltenbach, G.; Geny, B.; Lang, P.O. Effect of aerobic training on peak oxygen uptake among seniors aged 70 or older: A meta-analysis of randomized controlled trials. Rejuvenation Res. 2018, 21, 341–349. [Google Scholar] [CrossRef]
- Bouaziz, W.; Vogel, T.; Schmitt, E.; Kaltenbach, G.; Geny, B.; Lang, P.O. Health benefits of aerobic training pro-grams in adults aged 70 and over: A systematic review. Arch. Gerontol. Geriatr. 2017, 69, 110–127. [Google Scholar] [CrossRef] [PubMed]
- Aggarwal, A.; Ades, P.A. Exercise rehabilitation of older patients with cardiovascular disease. Cardiol. Clin. 2001, 19, 525–536. [Google Scholar] [CrossRef]
- Fleg, J.L. Can exercise conditioning be effective in older heart failure patients? Hear. Fail. Rev. 2002, 7, 99–103. [Google Scholar] [CrossRef]
- Huang, G.; Wang, R.; Chen, P.; Huang, S.C.; Donnelly, J.E.; Mehlferber, J.P. Dose-response relationship of cardi-orespiratory fitness adaptation to controlled endurance training in sedentary older adults. Eur. J. Prev. Cardiol. 2016, 23, 518–529. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions; Wiley: New York, NY, USA, 2011. [Google Scholar]
- Slimani, M.; Ramirez-Campillo, R.; Paravlic, A.; Hayes, L.D.; Bragazzi, N.L.; Sellami, M. The effects of physical training on quality of life, aerobic capacity, and cardiac function in older patients with heart failure: A meta-analysis. Front. Physiol. 2018, 9, 1564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhea, M.R.; Alvar, B.A.; Burkett, L.N.; Ball, S.D. A Meta-analysis to determine the dose response for strength development. Med. Sci. Sports Exerc. 2003, 35, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Assink, M.; Wibbelink, C.J.M. Fitting three-level meta-analytic models n R: A step-by-step tutorial. Quant. Methods Psychl. 2016, 12, 154–174. [Google Scholar] [CrossRef] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2018; Available online: https://www.R-project.org/ (accessed on 10 November 2020).
- RStudio Team. RStudio: Integrated Development for R.; RStudio, Inc.: Boston, MA, USA, 2019; Available online: http://www.rstudio.com/ (accessed on 10 November 2020).
- Viechtbauer, W. Package ‘Metafor’. Available online: https://cran.rproject.org/web/packages/metafor/metafor.pdf (accessed on 31 May 2019).
- Knapp, G.; Hartung, J. Improved tests for a random effects meta-regression with a single covariate. Stat. Med. 2003, 22, 2693–2710. [Google Scholar] [CrossRef]
- Kitzman, D.W.; Brubaker, P.H.; Herrington, D.M.; Morgan, T.M.; Stewart, K.P.; Hundley, W.G.; Abdelhamed, A.; Haykowsky, M.J. Effect of endurance exercise training on endothelial function and arterial stiffness in older patients with heart failure and preserved ejection fraction: A randomized, controlled, single-blind trial. J. Am. Coll. Cardiol. 2013, 62, 584–592. [Google Scholar] [CrossRef]
- Lovell, D.I.; Cuneo, R.; Gass, G.C. Can aerobic training improve muscle strength and power in older men? J. Aging Phys. Act. 2010, 18, 14–26. [Google Scholar] [CrossRef] [Green Version]
- Lovell, D.I.; Cuneo, R.; Wallace, J.; McLellan, C. The hormonal response of older men to sub-maximum aerobic exercise: The effect of training and detraining. Steroids 2012, 77, 413–418. [Google Scholar] [CrossRef] [PubMed]
- Buchner, D.M.; Cress, M.E.; De Lateur, B.J.; Esselman, P.C.; Margherita, A.J.; Price, R.; Wagner, E.H. The effect of strength and endurance training on gait, balance, fall risk, and health services use in community-living older adults. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 1997, 52, M218–M224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Babcock, M.; Paterson, D.H.; Cunningham, D. Effects of aerobic endurance training on gas exchange kinetics of older men. Med. Sci. Sports Exerc. 1994, 26, 447–452. [Google Scholar] [CrossRef] [PubMed]
- Coker, R.H.; Hays, N.P.; Williams, R.H.; Brown, A.D.; Freeling, S.A.; Kortebein, P.M.; Sullivan, D.H.; Starling, R.D.; Evans, W.J. Exercise-induced changes in insulin action and glycogen metabolism in elderly adults. Med. Sci. Sports Exerc. 2006, 38, 433–438. [Google Scholar] [CrossRef] [Green Version]
- Coker, R.H.; Williams, R.H.; Kortebein, P.M.; Sullivan, D.H.; Evans, W.J. Influence of exercise intensity on abdominal fat and adiponectin in elderly adults. Metab. Syndr. Relat. Disord. 2009, 7, 363–368. [Google Scholar] [CrossRef]
- DiPietro, L.; Seeman, T.E.; Stachenfeld, N.S.; Katz, L.D.; Nadel, E.R. Moderate-intensity aerobic training improves glucose tolerance in aging independent of abdominal adiposity. J. Am. Geriatr. Soc. 1998, 46, 875–879. [Google Scholar] [CrossRef]
- Probart, C.; Notelovitz, M.; Martin, D.; Khan, F.; Fields, C. The effect of moderate aerobic exercise on physical fitness among women 70 years and older. Maturitas 1991, 14, 49–56. [Google Scholar] [CrossRef]
- Wisloff, U.; Stoylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, O.; Haram, P.M.; Tjønna, A.E.; Jan, H.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef] [Green Version]
- Hagberg, J.M.; Graves, J.E.; Limacher, M.; Woods, D.R.; Leggett, S.H.; Cononie, C.; Gruber, J.J.; Pollock, M.L. Cardiovascular responses of 70-to 79-yr-old men and women to exercise training. J. Appl. Physiol. 1989, 66, 2589–2594. [Google Scholar] [CrossRef]
- Kallinen, M.; Sipilä, S.; Alen, M.; Suominen, H. Improving cardiovascular fitness by strength or endurance training in women aged 76–78 years. A population-based, randomized controlled trial. Age Ageing 2002, 31, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Raudenbush, S.W.; Hunter, J.E.; Schmidt, F.L. Methods of Meta-Analysis: Correcting Error and Bias in Research Findings. J. Am. Stat. Assoc. 1991, 86, 242. [Google Scholar] [CrossRef]
- Green, J.S.; Crouse, S.F. The effects of endurance training on functional capacity in the elderly: A meta-analysis. Med. Sci. Sports Exerc. 1995, 27, 920–926. [Google Scholar] [CrossRef] [PubMed]
- Huang, G.; Gibson, C.A.; Tran, Z.V.; Osness, W.H. Controlled endurance exercise training and VO2peak changes in older adults: A meta-analysis. Prev. Cardiol. 2005, 8, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Jones, A.M.; Carter, H. The effect of endurance training on parameters of aerobic fitness. Sports Med. 2000, 29, 373–386. [Google Scholar] [CrossRef]
- Spina, R.J.; Ogawa, T.; Kohrt, W.M.; Martin, W.H.; Holloszy, J.O.; Ehsani, A.A. Differences in cardiovascular adaptations to endurance exercise training between older men and women. J. Appl. Physiol. 1993, 75, 849–855. [Google Scholar] [CrossRef]
- Mandigout, S.; Lecoq, A.M.; Courteix, D.; Guenon, P.; Obert, P. Effect of gender in response to an aerobic training programme in prepubertal children. Acta Paediatr. 2001, 90, 9–15. [Google Scholar] [CrossRef]
- Murphy, W.G. The sex difference in haemoglobin levels in adults—Mechanisms, causes, and consequences. Blood Rev. 2014, 28, 41–47. [Google Scholar] [CrossRef]
- Song, H.-J.; Oh, S.; Quan, S.; Ryu, O.H.; Jeong, J.-Y.; Hong, K.-S.; Kim, D.-H. Gender differences in adiponectin levels and body composition in older adults: Hallym aging study. BMC Geriatr. 2014, 14, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wells, C.L. Women, Sport, and Performance: A Physiological Perspective. Med. Sci. Sports Exerc. 1992, 24, 277–278. [Google Scholar] [CrossRef]
- Milanović, Z.; Sporiš, G.; Weston, M. Effectiveness of high-intensity interval training (HIT) and continuous en-durance training for VO2peak improvements: A systematic review and meta-analysis of controlled trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine. American college of sports medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American college of sports medicine and the American heart association. Med. Sci. Sports Exerc. 2007, 39, 1423. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Independent Variables | Number of Studies | Number of Effect Size | SMD Estimate | SE | 95% CI | p | Heterogeneity, Q Statistic (p Value) | F Value and (p) between Groups |
|---|---|---|---|---|---|---|---|---|
| Main effect | ||||||||
| Pooled effect (REML model) | 12 | 18 | 2.60 | 0.79 | 0.97to 4.31 | 0.004 | 127.810 (<0.001) | NA |
| Health status | ||||||||
| Healthy | 6 | 9 | 2.25 | 0.51 | 1.09 to 3.04 | <0.001 | 74.91 (<0.001) | F1,15 = 13.52 (<0.001) |
| Unhealthy | 5 | 8 | 1.53 | 0.53 | 0.41 to 2.65 | 0.011 | ||
| Both (Healthy and Unhealthy) | 1 | 1 | 15.00 | 2.54 | 9.62 to 20.37 | <0.001 | ||
| Gender | ||||||||
| Both (Female and Male) | 7 | 10 | 1.38 | 0.91 | −0.54 to 3.30 | 0.148 | 91.94 (<0.001) | F1,15 = 3.17 (0.07) |
| Female | 2 | 2 | 3.63 | 1.66 | 0.11 to 7.14 | 0.044 | 102.03 (<0.001) | F1,15 = 0.46 (0.63) |
| Male | 3 | 6 | 2.23 | 1.3 | −0.31 to 4.71 | 0.088 | 119.08 (<0.001) | F1,15 = 2.41 (0.12) |
| Training duration | ||||||||
| <13 weeks | 4 | 9 | 2.26 | 0.97 | 0.22 to 4.23 | 0.032 | 115.37 (<0.001) | F1,16 = 0.54 (0.47) |
| ≥13 weeks | 8 | 9 | 2.87 | 0.84 | 1.05 to 4.58 | 0.004 | ||
| Session duration | ||||||||
| 20–30 min | 2 | 2 | 1.32 | 2.13 | −3.19 to 5.84 | 0.544 | 77.17 (<0.001) | F1,15 = 1.01 (0.37) |
| 31–45 min | 6 | 11 | 3.58 | 1.05 | 1.27 to 5.76 | 0.005 | ||
| 46–65 min | 5 | 5 | 2.25 | 1.13 | −0.14 to 4.64 | 0.064 | ||
| Training frequency | ||||||||
| 3 per week | 9 | 13 | 2.89 | 1.01 | 0.71 to 5.00 | 0.012 | 123.67 (<0.001) | F1,16 = 0.11 (0.73) |
| 4–5 per week | 3 | 5 | 2.19 | 1.74 | −1.48 to 5.853 | 0.225 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheour, S.; Cheour, C.; Bragazzi, N.L.; Zou, L.; Paravlic, A.H.; Slimani, M.; Cheour, F. Dose-Response Relationship between Endurance Training Prescription Variables and Increases in Aerobic Performance of Healthy and Unhealthy Middle and Very Old Individuals Aged 70 Years and Older: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life 2021, 11, 121. https://doi.org/10.3390/life11020121
Cheour S, Cheour C, Bragazzi NL, Zou L, Paravlic AH, Slimani M, Cheour F. Dose-Response Relationship between Endurance Training Prescription Variables and Increases in Aerobic Performance of Healthy and Unhealthy Middle and Very Old Individuals Aged 70 Years and Older: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Life. 2021; 11(2):121. https://doi.org/10.3390/life11020121
Chicago/Turabian StyleCheour, Sarah, Chouaib Cheour, Nicola Luigi Bragazzi, Liye Zou, Armin H. Paravlic, Maamer Slimani, and Foued Cheour. 2021. "Dose-Response Relationship between Endurance Training Prescription Variables and Increases in Aerobic Performance of Healthy and Unhealthy Middle and Very Old Individuals Aged 70 Years and Older: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Life 11, no. 2: 121. https://doi.org/10.3390/life11020121